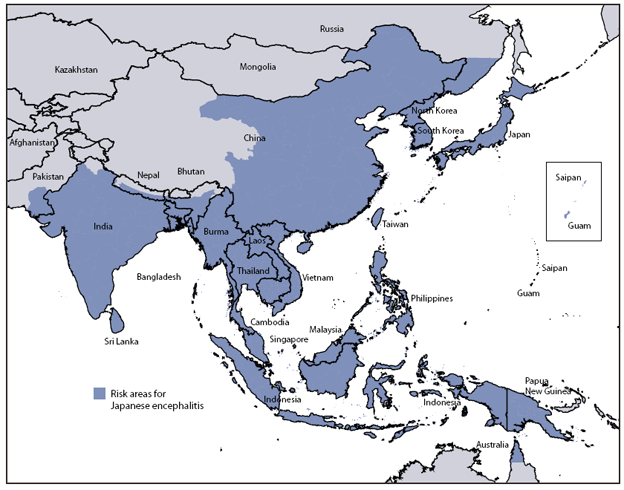
Geographic Japanese encephalitis: the risk areas are marked by darker shades of color. Click on the map if you want to enlarge it.
Image taken from Fischer M et al. MMWR 2010 Vol.59/RR-1
The recent marketing of new vaccine ' Japanese encephalitis from Vero cells (Vero Cell Culture-Derived JE Vaccine, JE-VC, strain SA14-14-2) I brought to mind a case report described three years ago by Peter Caramel and his group.
May 2007: a traveler just returned from Vietnam 49 years was admitted to the Hospital Amedeo di Savoia in Turin with a clinical picture characterized by high fever (39.5 ° C), disorientation, meningitis and other neurological signs. The EEG was pathological and magnetic resonance imaging documents the presence of lesions of the lentiform nucleus, right and left portion of the thalamus. Serology confirms an active infection by Japanese encephalitis virus (JEV, Japanese encephalitis virus). After treatment with intravenous immunoglobulin symptoms regressed and the patient was discharged, one month after discharge the patient appeared in good condition, except for a slight deficit of short-term memory.
What areas of Vietnam had been visited by the patient and for how long?
The patient between April 25 and May 16 had made a tour that included Ho Chi Minh, Hanoi, Halong Bay, Haipong, Mai Son, Dien Bien Phu, Sapa. Included a part of the rural areas and natural parks in the north. The arrangement had always been at the hotel. The patient had not received insect bites.
The patient had not been vaccinated: time the only vaccine against Japanese encephalitis was inactivated type, obtained from brain tissue of mice. However, the vaccine was not available in Italy, except in an ASL of Rome, and elsewhere in Europe was little used. Allergic reactions, mainly urticaria and angioedema, but sometimes severe reactions were reported with some frequency (a total of 180 to 640 casi/100.000 doses) and are 12-72 hours after administration, but sometimes after a few days. In addition, although very rarely, had been reported to ADEM (acute disseminated encephalomyelitis) temporally associated with the vaccine, it is a vaccine made from brain tissue, a possible causal relationship is biologically plausible ADEM, although the residual content of myelin in the final product was very low (\u0026lt;2 ng / ml).
It was therefore a vaccine with a safety profile is not optimal and that put limits to its acceptability among both health professionals and the public.
If a patient with the same itinerary of the case described by Pietro Caramello is today a center of Travel Medicine, health professionals should make it informed of the opportunity to get vaccinated?
I would say so. The vaccine is recommended for travelers to rural areas of endemic areas, particularly if they are permitted activities that include a prolonged outdoor exposure. The vaccine is also recommended for long stays (> 1 month) in endemic areas, irrespective of the route.
What is the risk of Japanese encephalitis in the traveler? What are the possible consequences of the disease?
The risk estimates found in literature are not uniform, either because they were drawn from heterogeneous populations and because the degree of risk varies according to region and, in some areas, even the season.
As for all the travelers who go to Asia, the risk appears very low (1 case / 1 million) are very different estimates for those who go to rural areas during the transmission period, I found estimates 1/5000/mese and even 1 / 5000 passengers per week. A recent review (GD Burchard et al. J Travel Med 2009, 16:204-216) reported on the basis of the interpolation attack rates observed during some epidemics, an estimate of 1/10.000/mese.
Danger areas are characterized by the simultaneous presence of the vector (Culex mosquitoes) and reservoir animals (pigs, water birds): mosquitoes, especially in many environments, you naturally want the intervention of ' man (growing rice), the abundance of water, keep circulating the virus in the animal reservoir, and occasionally can infect the human population.
The carrier stings usually outdoors (but it is also documented its activities in indoor environments) from the late afternoon and from dusk until dawn anyway. The rate of Culex mosquitoes infected with the virus is low (not more than 3%) and human cases with symptoms and signs of encephalitis are \u0026lt;1% of JEV infection.
Although this is an uncommon disease in traveler, give cause for concern is the high case fatality (20-30% of symptomatic cases) and the possibility of sequelae: 30-50% of patients have CNS sequelae even after years of illness.
what time of year is the transmission of the virus?
depends on latitude. In temperate areas of Asia the activity of JEV has a peak between May and December. In some tropical areas the transmission increases at the monsoon or rainy season, which have a distinctive pattern for each zone: for example, in South India the monsoon comes in different periods in the east coast and in the west, so also the same latitude as the period of risk of transmission of JEV is different. It follows that the health professional should know about, at least in broad terms, the climatic situation of each country to assess the risk depending on the itinerary of the traveler.
The new inactivated vaccine derived from Vero cells is effective and safe?
Effectiveness: the vaccine has been registered on the basis of serological correlate of protection as defined by WHO as the title neutralizing Ac > = 1:10. In clinical studies, seroconversion was observed in 96% of subjects at a distance of 56 days after the first dose. The cycle is two doses separated by an interval of 28 days. A booster dose is recommended at a distance of 12-24 months after the primary, before the potential new exposure to the virus.
Once you know the serological correlate of protection against a particular pathogen, the registration of a new vaccine can be demonstrated when, following vaccination, antibody response at or above the level considered protective. Of course, it is now necessary studies to know the effectiveness of the vaccine in the field (under field conditions).
Security: in clinical trials before registration of the vaccine have been reported headache (20%), myalgia (13%) and, more rarely, other systemic reactions (including asthenia and flu-like symptoms) or local (pain, edema, erythema) usually mild. These studies, of course, have been conducted on a restricted population, it requires careful post-marketing surveillance to detect rare and severe reactions.
When the vaccine is not is recommended in children and adolescents because they are not yet available data on safety and effectiveness in these age groups.
to write this post I used the following sources:
Caramello P, Canta F, Balbo R, F Lipani, Ariaudo S, De Agostini M, Calleri G, L Bogle, A. Di Caro A Case of Imported JE Acquired During Short Travel in Vietnam. Are Current Recommendations About Vaccination Broader? Journal of Travel Medicine 2007, 14:346-348
DOI: 10.1111/j.1708-8305.2007.00140.x
GD Burchard et al. Expert opinion on vaccination of travellers against Japanese Encephalitis. Journal of Travel Medicine 2009;16:204-216
DOI: 10.1111/j.1708-8305.2009.00330.x
M Fischer et al. Japanese Encephalitis Vaccines. Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR 2010 Vol.59/RR-1
Ixiaro. Riassunto delle product characteristics. http://www.ema.europa.eu/docs/it_IT/document_library/EPAR_-_Product_Information/human/000963/WC500037287.pdf
0 comments:
Post a Comment